People with BE are more susceptible to lung infections because damaged airways allow mucus to build up, creating an environment that promotes infection. While bacteria are the most common cause, viruses and fungi can also infect the lungs and contribute to flare-ups. The specific infections can vary from person to person, but some are more common in people with BE. Routine sputum tests that include culture and antibiotic sensitivity – looking for infections and determining which drugs may work on those infections – are a cornerstone of monitoring BE. One such test is an acid fast bacilli (AFB) test to identify nontuberculous mycobacteria. Other tests would look for fungal infection which may also need to be treated. Some types of fungi, including Aspergillus, can infect the lungs or trigger allergic reactions. Common aspergillus-related diseases affecting patients with BE include allergic Bronchopulmonary Aspergillosis (ABPA), chronic pulmonary aspergillosis (CPA), and aspergilloma. Viral infections (such as flu, common cold, or RSV) can also trigger exacerbations.
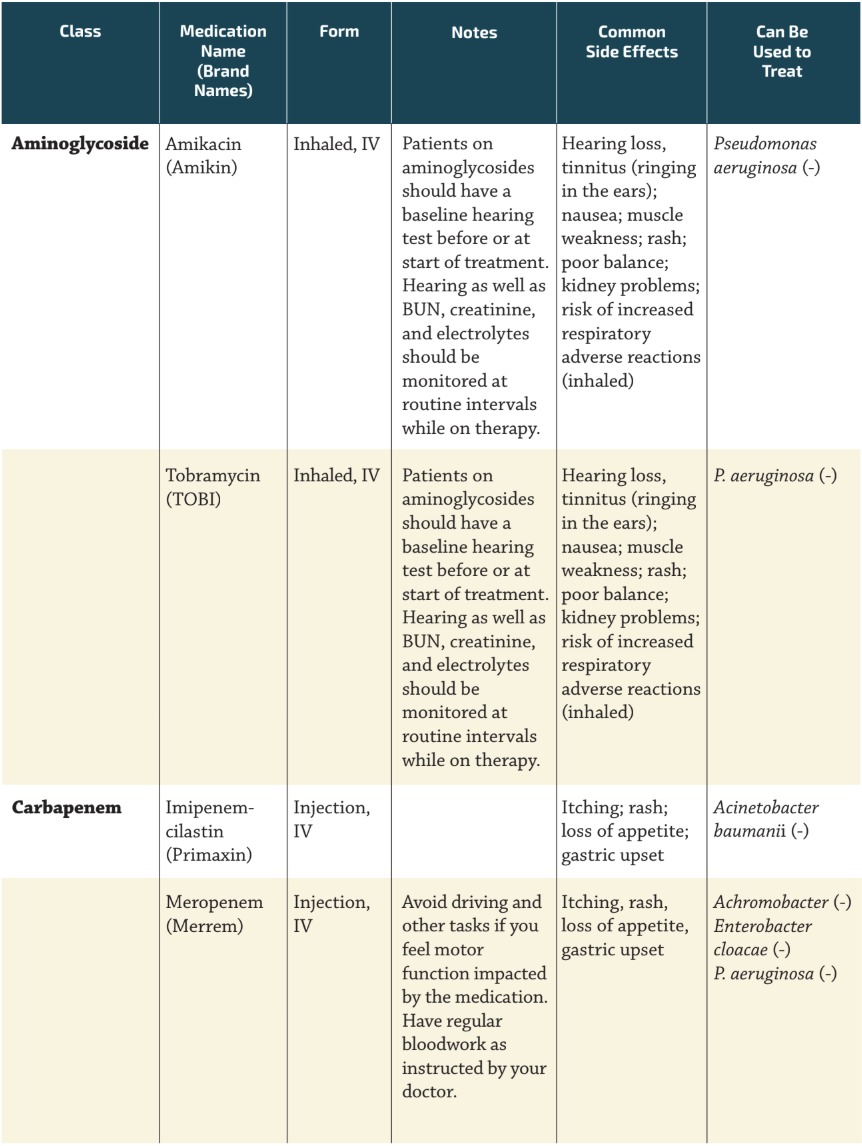
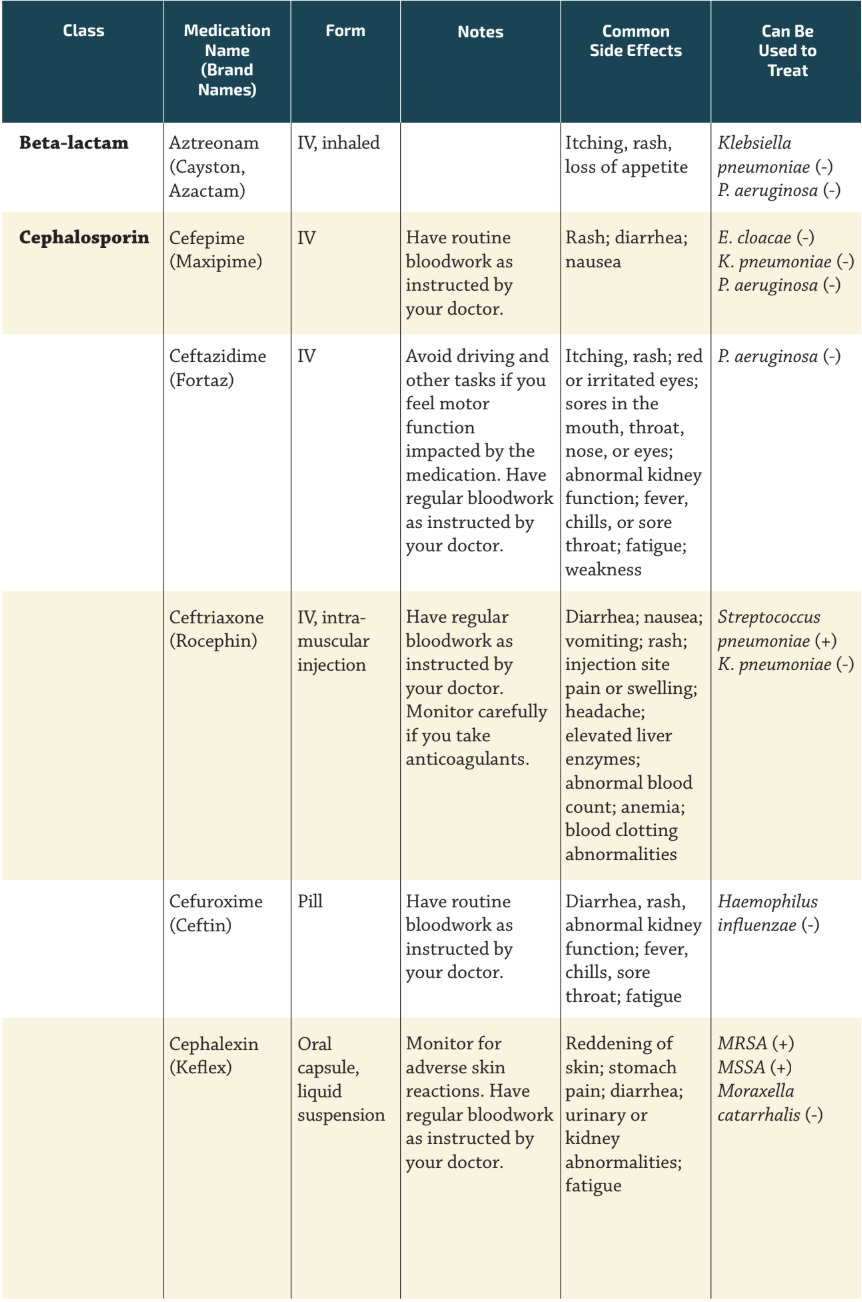
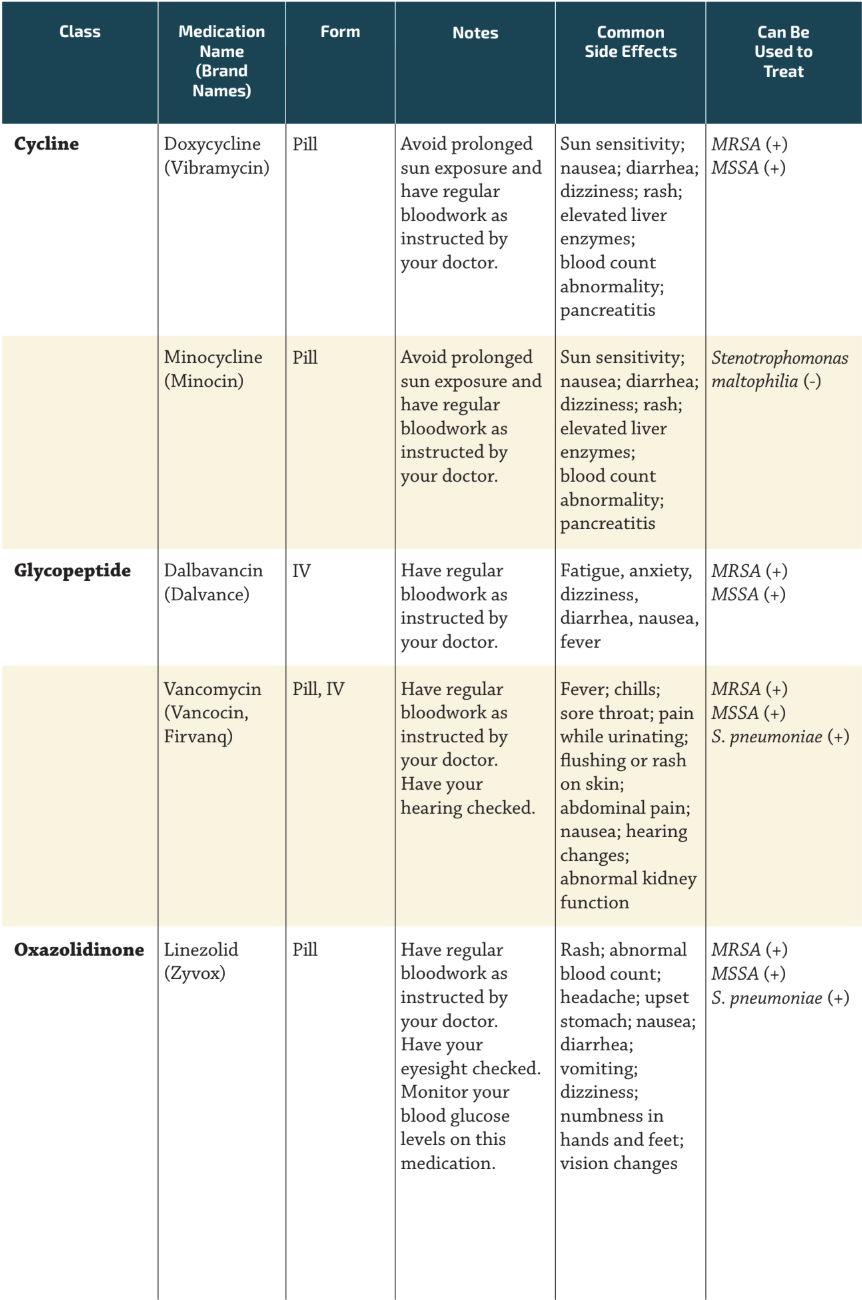
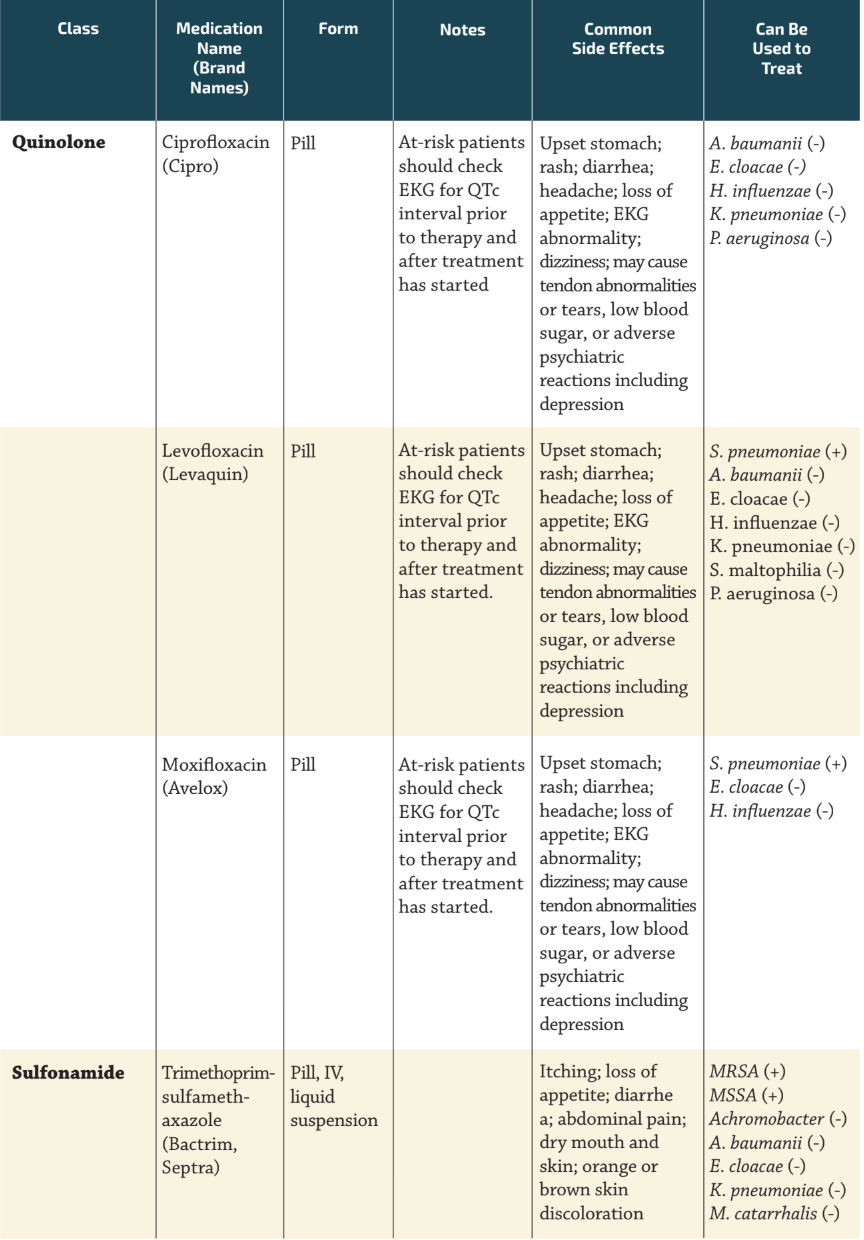
Bacterial Infections and Treatments The following chart covers some of the more common bacterial infections, but there are other germs that you may encounter and other treatments that may be used for you. The treatments here are examples of some of the drugs that can be used to treat these infections, but there are other options available that your care team may recommend, based on your specific infection and lab results.
Gram-positive bugs are indicated with (+) and gram-negative with (-). Bacteria are classified as either gram-positive or gram-negative based on a lab technique called the Gram stain, in which bacteria are treated with a series of dyes. Those with a thick outer cell wall retain a purple color (gram-positive), while those with a thinner wall and an extra outer membrane wash out to pink (gram-negative). This distinction helps doctors identify the type of bacteria causing an infection.
Note: “MSSA” stands for “methicillin-susceptible staphylococcus aureus.” “MRSA” stands for “methicillin-resistant staphylococcus aureus.” Where the Genus and species names are used, after its first appearance, the genus name will be abbreviated throughout the rest of this document.
For more information on nontuberculous mycobacteria (NTM) and medications used to treat them, visit ntminfo.org.
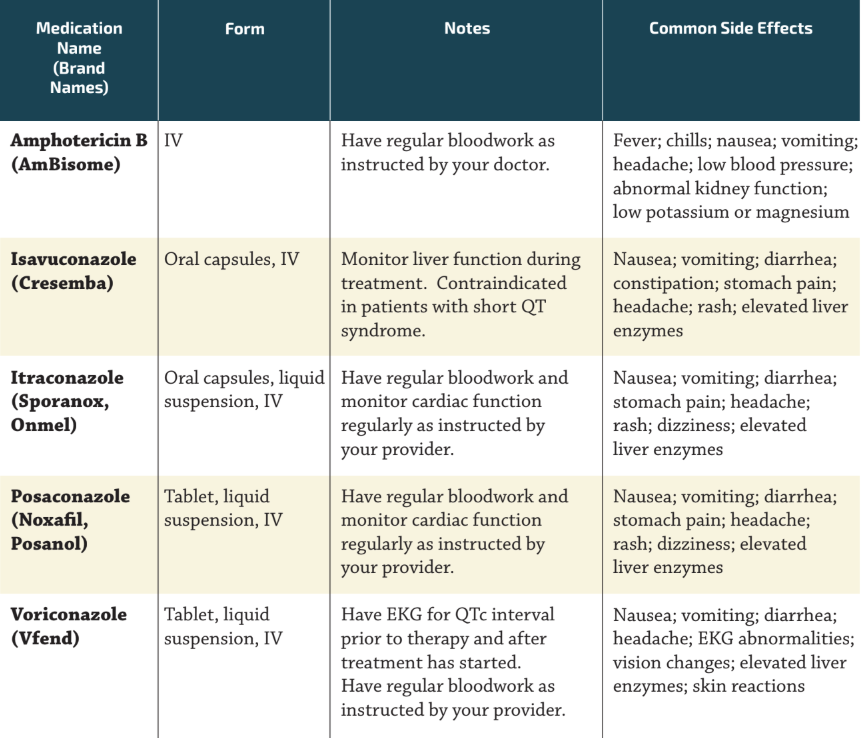
Fungal Infections and Treatments People with bronchiectasis are also more vulnerable to lung infections caused by fungal pathogens such as Aspergillus fumigatus, Exophiala spp., Trichosporon spp., and Scedosporium spp. Below are some of the anti-fungal treatments used to treat them.
Colonization vs. Infection Not every organism found in the airways causes an active infection. If someone is “colonized,” this means the infectious organism is somewhere in or on the body but is not causing symptoms. Some people with bronchiectasis carry bacteria or other organisms in their lungs long-term without feeling sick. This is called “asymptomatic infection.” Symptomatic infection, or disease, begins when the infectious organism enters the body and begins to replicate and cause symptoms. While colonizing organisms may not require treatment right away, identifying and monitoring them is important because they may turn into a symptomatic infection later on.
Testing for Infections To properly treat an infection, your providers need to know which organism is causing it. This begins with testing your sputum. Routine sputum testing is one of the most important aspects of managing bronchiectasis since organisms in the lungs can change over time. This testing should be repeated at regular intervals or when your symptoms change.
Sputum Collection Before testing can be done, a sputum sample needs to be collected. The preferred method is to cough up sputum and collect it in a sterile container. If you are unable to produce sputum on your own, there are several techniques that can help, including huff coughing, nebulized hypertonic saline treatments, and devices such as positive expiratory pressure (PEP) or high frequency chest wall oscillation devices. Once collected, the sample can be refrigerated overnight before being taken to the lab for testing. Another intervention to collect a sputum sample is bronchoscopy, where a thin, flexible tube with a tiny camera and light on the end is gently guided through your nose or mouth, down your throat, past your vocal cords, and into your airways. A saline rinse loosens mucus that is then suctioned out as your sample. You will be given a sedative and a numbing spray beforehand. The procedure typically takes 30–60 minutes, after which your throat may feel temporarily sore or numb.
Lab Testing and Culturing After the sputum sample reaches the lab, it is tested using a process called a culture. This process allows laboratory professionals to identify any bacteria, fungi, or other organisms already present in the sample. If organisms are identified, the results help providers choose the most effective treatment and avoid unnecessary antibiotics.